Emergency Medicine
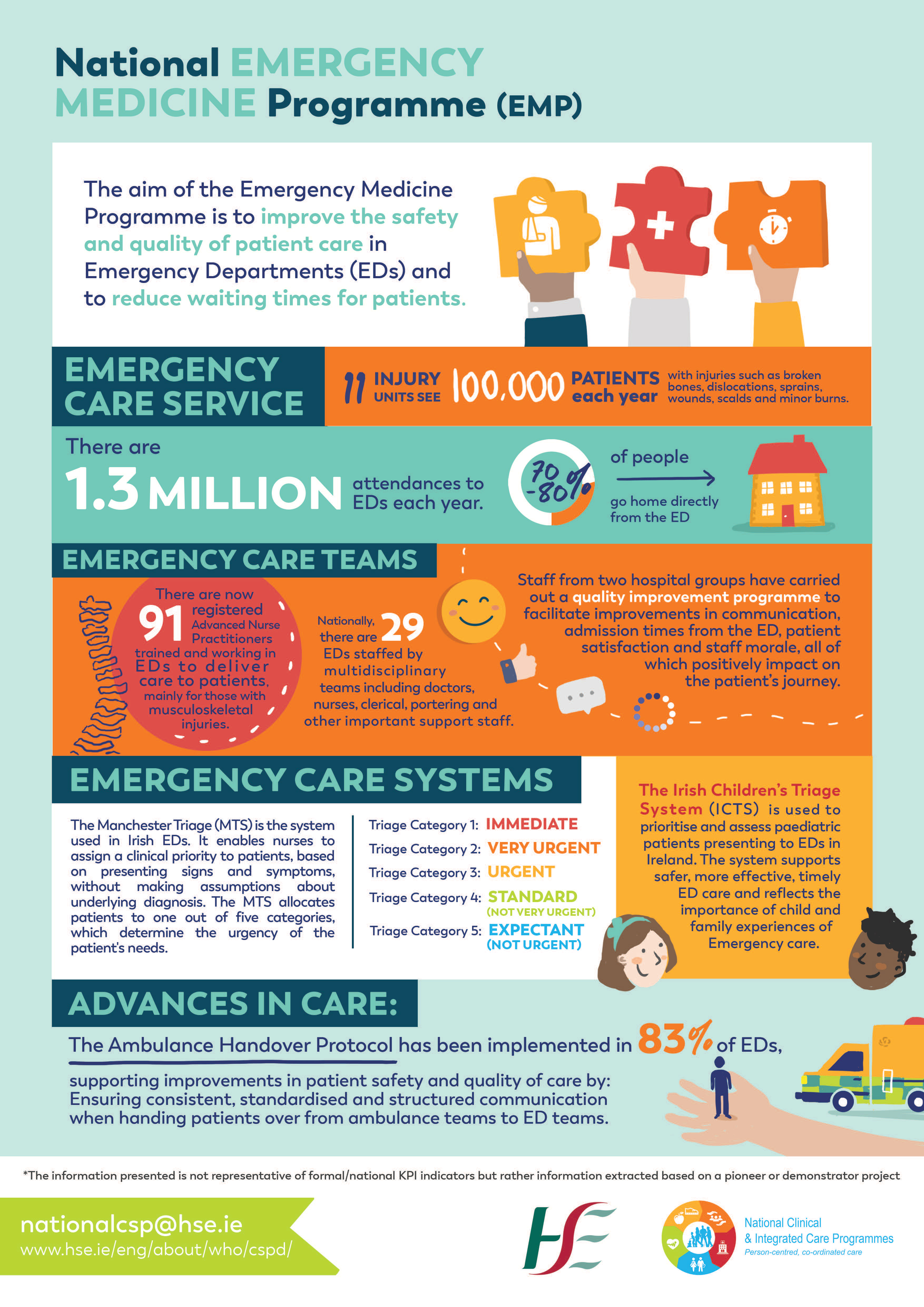
The aim of the Emergency Medicine Programme (EMP) is to improve the safety and quality of patient care in emergency departments (EDs) and injury units (IU) to reduce waiting times for patients and keep care as close to home as possible.
The EMP is led by a multidisciplinary working group that includes consultants in emergency medicine, emergency nurses, representatives of pre-hospital care and the therapy professions. It is supported by the Irish Committee for Emergency Medicine Training, the Irish Association for Emergency Medicine, the Office of the Nursing and Midwifery Services Director, the HSCP Office (Health and Social Care Professions) and Clinical Design and Innovation of the HSE.
Watch the Launching the Future of Emergency Care webinar here or learn more about the EMP on the EMNOW website.
- National Clinical Lead: Dr Rosa McNamara
- National Programme Managers: Mary Flynn and Breda Naddy
- National Nurse Lead: Dr Sarah Watkins
- National Administrators and Project Support: Sinead Reilly and Fiona Brazil
National Working Group
- Michelle Barlow, Advanced Nurse Practitioner, Midland Regional Hospital Tullamore
- Dr Carol Blackburn, Consultant in Emergency Medicine, Children's Health Ireland (CHI) at Crumlin
- Fiona Brazil, National Administrator and Project Support, National Emergency Medicine Programme
- Dr Emma-May Curran, IEMTA President, Specialist Registrar in Emergency Medicine
- Dr Conor Deasy, Consultant in Emergency Medicine, Cork University Hospital, President of IAEM (Irish Association for Emergency Medicine)
- Dr James Foley, Consultant in Emergency Medicine University Hospital Galway
- Mary Flynn, National Programme Manager, National Emergency Medicine Programme
- Dr Aine Keating, Consultant in Emergency Medicine Letterkenny University Hospital
- Dr Orla Kelly, Consultant in Emergency Medicine, University Hospital Waterford
- Regina Lee, Senior Clinical Pharmacist University Hospital Limerick
- Dr Elizabeth Little, Consultant in Emergency Medicine Mater Private Network
- Dr Gerry McCarthy, Consultant in Emergency Medicine, Cork University Hospital
- Kara McLoughlin, Occupational tharapist, Research Fellow/PhD Candidate Ageing Research Centre/School of Allied Health University of Limerick
- Stephen McMahon, Co-Founder & Director of the Irish Patients' Association (IPA)
- Dr Rosa McNamara, Consultant in Emergency Medicine, St Vincent’s Hospital, Clinical Lead, National Emergency Medicine Programme
- Dr Michael Molloy, Consultant Geriatrician Cork University Hospital, National Clinical Advisor Acute Operations
- Dr Anna Moore, Consultant in Emergency Medicine, Midland Regional Hospital Tullamore
- Dr Jeffery Mulcaire, Consultant Emergency Medicine, St James's Hospital.
- Dr Caitriona Mullarkey, Consultant in Emergency Medicine UHL
- Breda Naddy, National Programme Manager, National Emergency Medicine Programme
- Sinead Reilly, National Administrator and Project Support, National Emergency Medicine Programme
- Dr Nikita Svirkov-Vainberg, Consultant in Emergency Medicine Our Lady of Lourdes Hospital
- Dr Calum Patrick Swift, Consultant in Emergency Medicine University Hospital Galway
- Aoife Synnott, Clinical Specialist Physiotherapist Older Persons, University Hospital Limerick
- Katy Twomey, Principal Social Worker at Cork University Hospital
- Dr Sarah Watkins, EMP National Nurse Lead, RANP in Unscheduled Care Acute Medicine
The team can be contacted at emp@rcsi.ie.
Older Adults QIF
A national Quality Improvement Framework (QIF) provides a standardised yet adaptable approach to improving older adult care. Early implementation across EDs and IUs demonstrates improved assessment, patient experience and workflow efficiency. It supports earlier identification of high-risk patients and more consistent delivery of essential care, even in resource-constrained settings.
Haemoptysis
The development of a national, multidisciplinary clinical consensus guideline for the emergency management of haemoptysis is underway. This will allow standardization of triage, initial management, imaging, definite hemorrhage control and pathways for transfer in order to reduce morbidity and mortality.
Green Emergency Medicine
Supported by Spark Innovation Funding, four sites have achieved Bronze accreditation through the Royal College of Emergency Medicine’s GreenED framework with seven more actively progressing toward Bronze and Silver accreditation. Multidisciplinary Green Teams implemented interventions including waste audits, sustainable prescribing, energy reduction and education initiatives. Cross-site collaboration, shared learning and national policy engagement support frontline sustainability practices. An e‑learning module has been developed in partnership with HSE Climate and Sustainability.
Triage QIP implementation
Webinars are being delivered by Dr Sarah Watkins, Nurse Lead, NCP EM to support Triage QIP implementation which is intended to reform triage and assist staff with timely patient prioritisation and post triage care. Five webinars are scheduled and a pre-recorded version will be available on this website. The QIP has been disseminated to the regions and Triage QIP Steering Committees have been established in sites nationally. A review of progress with regard to Triage QIP implementation will take place to determine need for further webinars and additional training. The Triage QIP will be audited in 2027. If you would like to attend the webinar, please visit the HSE website.
HIRAID Emergency Nursing Assessment Framework
A pilot study is underway in Mercy University Hospital. This Spark funded project will trial the HIRAID Emergency Nursing Assessment Framework which is the only validated tool for use in the Post Triage Phase of Care. The Mercy pilot represents the first time that this framework is being tested in the Irish context. Pre-implementation work in advance of July rollout is underway and the Australian expert team were onsite in the Mercy Hospital to facilitate instructor programme and co-designed rollout.
Digital EMEWS
In 2025, Digital EMEWS was piloted in Irish EDs as part of a national strategy to enhance patient safety through digital transformation. Early implementation of Digital EMEWS in Irish EDs suggests significant potential to improve patient safety, situational awareness, and clinical workflow. Successful adoption is dependent on strong clinical leadership, staff engagement, and integration into existing practices. A proposal mandate for the national roll-out of Digital EMEWS is underway.
Paediatric Emergency Medicine Strategy
The pathways for children in EDs has been mapped for all 17 sites that see both adults and children. Focus groups and steering group engagement have informed next steps and a Spark-supported design-led approach will develop evidence-based recommendations.
Children’s Early Warning System (C‑EMEWS)
An options appraisal is underway informed by updated literature research. Engagement with HRB CICER has commenced to support evidence-based decision-making on the development of a national Children’s Early Warning System in emergency care settings.
EM Nursing Groups
Sarah Watkins, Nurse Lead, NCP EM has convened an overarching group from the NCP EM nursing subgroups to inform NCP EM strategic planning and set an emergency nursing direction for patient care. Regular engagement with emergency nursing groups continues every six weeks, ensuring frontline issues inform programme planning and feed back to the RDONMs.
Mental Health Transfer Guidance
A multidisciplinary, multi-agency Mental Health Transport Group has been formed to review the 2013 guide to assist matching staff clinical level and mode of transport with the care needs of patients with mental health problems in the Emergency Department. Review of existing guidance is underway, with gaps and risks being identified.
Injury Unit Education and Certification Framework
The development of a foundation programme with the support of the RDONMs has been approved for QQI accreditation. A curriculum development team will meet in the coming weeks with a view to having a Level 8 Foundation Programme in Injury Unit Nursing available for rollout in 2027.
Pharmacy in Unscheduled Care
A collaboration with the Department of Health and the Health Research Board has been established to undertake an evidence synthesis on the role of pharmacy in EDs.
Domestic Sexual and Gender Based Violence
This national QI framework establishes a practical, trauma-informed model for integrating DSGBV identification and response into routine emergency care. Its tiered, scalable design supports widespread adoption and sustainability. Embedding DSGBV care within EDs and IUs has the potential to improve patient outcomes, safety and dignity at a population level. Building on the published DSGBV QIP, a national video-based training programme is being explored.
HSCP presence in EDs
In recent years, there is a growing presence of HSCP staff within our EDs. The EMP are in the process of mapping the presence of these HSCP's and recording the various programmes available nationally. This will allow collaboration between our hospitals and allow staff development in order to advance practice of staff in fulfilling their role in this area.
{kind=link}